EXTERNAL LINK
You are about to leave Pajunk.com. This link is provided strictly for information sharing purposes.
Pajunk GmbH assumes no responsibility for the quality, content, nature, or reliability of any linked site.

The unique design of the Sprotte needle has made it a success. This design has revolutionised spinal anaesthesia. Pajunk is proud to have taken this step together with Prof. Sprotte.
Milestones of the Sprotte:
1979 - Launch
1980 - break trough in regional anaesthesia
In 1980’s - First studies confirming the concept of the Sprotte needle repeatedly. Thus increasing interest.
1990 - Scientific success of the needle - first comparative studies with Quincke & Whitacre needle. This led to the Sprotte needle with its atraumatic tip geometry becoming the new standard in anaesthesia in some parts of the world market.
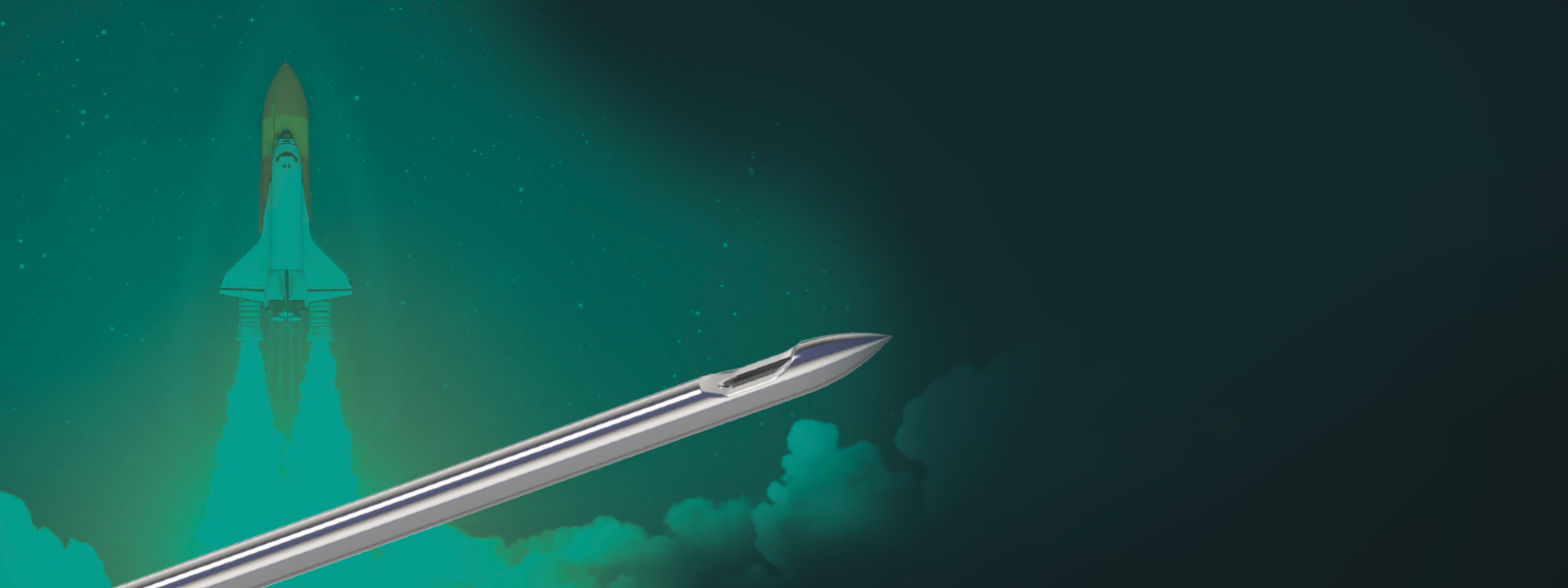
However, what is so revolutionary about our Sprotte?
Atraumtic Tip Design
Lateral Eye
Optimal Lateral Eye Size and Placement
Precision-Ground Metal Stylet
Further, the Sprotte needle has also revolutionised the lumbar puncture area.
In comparison with the Qunicke tip needles, the Sprotte needles has an Evidence class 1, recommendation level A8,9,10,11 in the sector of lumbar puncture
The conclusion out of different studies: “It’s time to change the needle.”4,5,14 for lumbar puncture.
1 Saenghirunvattana R. et al. A comparison study between newly-designed pencil-point and cutting needles in spinal anesthesia, J. Med. Assoc. Thai. 2008; 91 (Suppl 1): S156–161
2 Armon C., Evans R. W. Addendum to assessment: Prevention of postlumbar puncture headaches Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology., Neurology., 2005; 65; 510
3 Cesarini, M. et al. Sprotte needle for intrathecal anaesthesia for Caesarean section: incidence of postdural puncture headache., Aaesthesia 1990; 45: 646–658
4 Davis, A.; Dobson, R.; Kaninia, S.; Giovannoni, G.; Schmierer, K. (2016): Atraumatic needles for lumbar puncture: why haven't neurologists changed? In Practical neurology 16 (1), pp. 1822. DOI: 10.1136/practneurol-2014-001055.0
5 Engedal, Thorbjørn S.; Ørding, Helle; Vilholm, Ole Jakob (2015): Changing the needle for lumbar punctures: results from a prospective study. In Clinical neurology and neurosurgery 130, pp. 7479. DOI: 10.1016/j.clineuro.2014.12.020.
6 Tung, C. E.; Yuen, T. S.; Lansberg, M. G. (2012): Cost comparison between the atraumatic and cutting lumbar puncture needles. In Neurology 78, pp. 109113.
7 Arevalo-Rodriguez, Ingrid; Muñoz, Luis; Godoy-Casasbuenas, Natalia; Ciapponi, Agustín; Arevalo, Jimmy J.; Boogaard, Sabine; Roqué I Figuls, Marta (2017): Needle gauge and tip designs for preventing post-dural puncture headache (PDPH). In The Cochrane database of systematic reviews 4, CD010807. DOI: 10.1002/14651858.CD010807.pub2.
8 McLaughlin, Colleen A.; Hockenberry, Marilyn J.; Kurtzberg, Joanne; Hueckel, Rémi; Martin, Paul L.; Docherty, Sharron L. (2014): Standardization of health care provider competencies for intrathecal access procedures. In Journal of pediatric oncology nursing: official journal of the Association of Pediatric Oncology Nurses 31 (6), pp. 304316. DOI: 10.1177/1043454214543019.
9 Nath, Siddharth; Koziarz, Alex; Badhiwala, Jetan H.; Alhazzani, Waleed; Jaeschke, Roman; Sharma, Sunjay et al. (2018): Atraumatic versus conventional lumbar puncture needles: a systematic review and meta-analysis. In The Lancet 391 (10126), pp. 11971204. DOI: 10.1016/S0140-6736(17)32451-0.
10 Rochwerg, Bram; Almenawer, Saleh A.; Siemieniuk, Reed A. C.; Vandvik, Per Olav; Agoritsas, Thomas; Lytvyn, Lyubov et al. (2018): Atraumatic (pencil-point) versus conventional needles for lumbar puncture: a clinical practice guideline. In BMJ, k1920. DOI: 10.1136/bmj.k1920.
11 Zhang, Yi C.; Chandler, Alexander J.; Kagetsu, Nolan J. (2014): Technical compliance to standard guidelines for lumbar puncture and myelography: survey of academic neuroradiology attendings and fellows. In Academic radiology 21 (5), pp. 612616. DOI: 10.1016/j.acra.2014.01.021.
12 Bellamkonda, Venkatesh R.; Wright, Thomas C.; Lohse, Christine M.; Keaveny, Virginia R.; Funk, Eric C.; Olson, Michael D.; Laack, Torrey A. (2017): Effect of spinal needle characteristics on measurement of spinal canal opening pressure. In The American journal of emergency medicine 35 (5), pp. 769772. DOI: 10.1016/j.ajem.2017.01.047.
13 Puolakka, R.; Andersson, L. C.; Rosenberg, H. (2000): Microscopic Analysis of Threee Different Spinal Needle Tips After Experimental Subarachnoid Puncture. In Regional Anesthesia and Pain Medicine 25 (2), pp. 163169.
14 Lavi R., Rowe J.M., Avivi I. Lumbar Puncture. It Is Time to Change the Needle, Eur Neurol, 2010; 64:108113